Hotal Traditional Oriental Medicine Letters HTOML
![Hotal Traditional Oriental Medicine Letters [HTOML]](../HARI/img/htoml_es.jpg)
Vol.12, No.1, 2025
 0.4M
0.4M
Acupuncture and Moxibustion Treatment for Prevention of Cystitis
Nobuyuki Otsuka Affiliation Address
Keywords: cystitis, prevention, liver deficiency pattern, eight confluent points, warm-tube moxibustion, lifestyle guidance, oriental medicine, acupuncture and moxibustion
Cystitis is more common in women, and it is estimated that approximately half of all women experience one to two episodes during their lifetime. In contrast, it is rare in men in the absence of underlying diseases. Cystitis is defined as inflammation of the bladder caused by bacterial infection and is broadly classified into acute cystitis and chronic cystitis [1]. Acute cystitis is more common and is typically caused by ascending infection of gram-negative bacilli, including Escherichia coli, from the external genitalia through the urethra. In cases with underlying diseases, cystitis tends to recur and may become refractory [2]. In cases of recurrent cystitis, antibiotic resistance may develop, making antibiotics less effective and limiting the range of antibiotics that can be used [3]. Therefore, this study aimed to prevent cystitis and improve the patient's constitution to make them less susceptible to cystitis through acupuncture treatment, thereby avoiding the need for antibiotic therapy.
The main symptoms of cystitis include urinary frequency, dysuria, a sensation of residual urine, cloudy urine, and hematuria. The diagnosis of cystitis is based on the presence of urinary frequency, dysuria, and cloudy urine, and is confirmed by urinalysis and urine culture. Treatment typically involves the administration of antibiotics. Acute uncomplicated cystitis without underlying disease is generally cured relatively easily with antibiotic therapy. If the causative organism is susceptible, a 3-day course of antibiotics is sufficient to achieve adequate therapeutic effects, and even a 1-day or single-dose regimen may be effective. If symptoms and urinary findings do not improve after 3 days of treatment, the antibiotic should be changed. If there is no response after 7 days of treatment, complicated cystitis associated with underlying urinary tract disorders should be considered. In patient education, rest is first recommended. Patients are instructed to drink plenty of fluids, not hold their urine, and keep their genital area clean to promote self-cleaning through diuresis. During active infection, patients should refrain from sexual intercourse, avoid irritative foods and beverag
es such as alcohol, and maintain adequate warmth [4].
In traditional Chinese medicine (TCM), the primary cause of cystitis is considered to be a deficiency of the kidney, leading to the accumulation of damp-heat in the lower burner and dysfunction of the bladder’s qi transformation [5]. The kidney and bladder are internally-externally related and mutually influence each other. If the condition persists over a long period without resolution, kidney yin or kidney yang may become impaired, resulting in a mixed pattern of deficiency and excess. The treatment principle for cystitis is to restore the bladder’s qi transformation and to clear damp-heat from the lower burner. The commonly used acupoints for acupuncture treatment are BL23, BL28, CV3, and SP6, with additional points including BL32 and LR8. Treatment is typically administered daily, with one session per day, with 5-10 sessions constituting one course. Moderate to strong stimulation is applied, using the intermittent needle manipulation technique. In this technique, after the needle reaches the intended depth, it is partially withdrawn and retained for a short period, then reinserted to the original depth and retained again; this process is repeated. The rationale for point selection is as follows. BL23 is the Back-Shu point of the kidney and regulates kidney qi and promotes water metabolism. BL28 is the Back-Shu point of the bladder. CV3 is the Front-Mu point of the bladder, where the three yin meridians of the foot intersect with the Conception Vessel in the lower abdomen. SP6 is the intersection point of the three yin meridians of the foot. Therefore, the combination of SP6 and CV3, with BL28 as an adjunct, can clear damp-heat from the bladder and facilitate qi transformation in the lower burner. BL32 belongs to the Foot Taiyang meridian and is located adjacent to BL28, exhibiting similar therapeutic effects. LR8 is the He-Sea point of the Foot Jueyin meridian; this meridian ascends to the genital region and lower abdomen and has the function of clearing damp-heat from the lower burner. The above describes a treatment approach for cystitis rather than its prevention. However, as TCM emphasizes preventive medicine, it is considered that continuous acupuncture treatment aimed at restoring bladder qi transformation and clearing damp-heat from the lower burner may contribute to the prevention of cystitis.The literature on cystitis in Japanese acupuncture is listed as follows. In Commentary on Valuable Records on Acupuncture and Moxibustion, the acupoints indicated for treatment are as follows: for acupuncture, CV4, GB43, and SP6; for moxibustion, BL23, BL28, BL27, BL33, SP6, CV8, and CV5 [6]. In Essence of Acupuncture and Moxibustion, the acupoints described for bladder pain include CV4 or CV3, and CV6 [7]. In Medical Dictionary of Acupuncture and Moxibustion, the listed acupoints are CV6, BL23, BL25, BL27, SP14, BL51, BL52, BL26, GB20, BL18, BL20, BL28, GV9, Ex-B4, LR13, LR14, CV5, CV4, and ST25 [8]. In Medical Dictionary of Clinical Acupuncture and Moxibustion, the acupoints for cystitis are categorized as follows: local points include CV1, CV2, CV3, BL28, BL32, and KI11; adjacent points include LR11, LR10, LR9, LR8, SP10, and LR14; and circulatory points include BL4 and Upper-BL10 [9]. In Case Studies of Denmei Shudo, liver deficiency pattern is most frequently observed, with kidney deficiency and lung deficiency patterns also reported [10]. The acupoints used include CV6, CV4, and CV3 along the lower abdomen from CV2 to CV7; kidney meridian points KI12, KI13, and KI14; and, on the back, BL32, BL33, BL28, BL53, BL23, BL52, and Ex-B8. For the lower limbs, SP6, LR8, and BL59 are utilized. In moxibustion therapy, CV6, CV3, SP6 or LR8, BL23, and BL32 are employed. For preventive treatment, moxibustion on SP6, CV6, or CV3 are recommended. Additionally, classical texts describe urinary symptoms related to cystitis, such as dysuria and urinary difficulty, as well as impaired urination, ST27 is documented as a therapeutic point for urinary disorders [6,11,12].
A case is presented below. The patient was a 40-year-old woman. Her first visit was on Y day of February in year X. The chief complaint was cystitis. Regarding the present illness, the patient experienced her first episode of cystitis in year X-34. From year X-3, cystitis recurred at a frequency of once every 3-4 months. She had no underlying diseases, and given that the frequency of onset exceeded three episodes per year, she was considered to have recurrent cystitis characterized by repeated episodes of acute uncomplicated cystitis. Prodromal symptoms suggestive of cystitis occurred approximately once per month. At the hospital, antibiotics were prescribed, and symptoms resolved within approximately two weeks. However, repeated administration of antibiotics due to recurrence led to the development of drug resistance, necessitating changes in antibiotics each time. As the available antibiotic options became limited, she visited our clinic seeking acupuncture treatment to prevent cystitis without the use of antibiotics. During episodes of cystitis, she experienced discomfort and itching in the lower abdomen, which progressed to abdominal pain when inflammation developed. Precipitating factors included fatigue, exposure to cold, and inability to find the time to go to the toilet. Aggravating factors included reduced fluid intake, the onset of lower abdominal discomfort, and abdominal pain. Symptoms were alleviated by increased fluid intake. Additional complaints included tension on the right side of the back from the ninth to twelfth thoracic vertebrae, distension and pain in the epigastric and hepatic regions, poor gastric condition, and thirst with a desire to drink water.
On looking diagnosis, her height was 150 cm and weight was 50 kg, with a normal body build. Blood pressure was 110/70 mmHg, and the skin of the forearm appeared pale. On listening and smelling diagnoses, her voice was strong; in the five-tone system, she corresponded to shang, in the five voices to hu, while the five odors were undetermined. On asking diagnosis, the patient reported consuming two to three meals per day, with dinner taken between 9:00 and 10:00 PM, typically until full. She preferred sweet and spicy flavors. Sleep was satisfactory. Urination occurred five times per day, with one nocturnal episode. Bowel movements were normal, occurring once every one to two days. She did not smoke and occasionally consumed approximately 2 liters of beer. She exercised at a gym once or twice per week. She reported eye fatigue, perceived stress, and a tendency toward excessive rumination. She also complained of heaviness in the lower body. Her past medical history included seasonal allergic rhinitis and cough-variant asthma during winter. Current medications included vitamin C and probiotics. She had prior experience with acupuncture for the neck, shoulders, and lower back at an osteopathic clinic; however, she had no experience with comprehensive acupuncture treatment. She was familiar with moxibustion, as her mother had frequently used it. On touching diagnosis, the body was soft, with an impression of relatively high body fat. On abdominal diagnosis, the abdomen was generally distended. The upper abdomen showed tension, whereas the lower abdomen felt weak. The liver region was depressed and showed the greatest deficiency; the kidney region was also weak and the second most deficient. The lung and spleen regions were firm and tense, indicating excess, while the heart region was unremarkable. On pulse diagnosis, the pulse quality was sinking, moderate speed, and deficient. Comparative pulse diagnosis revealed that the liver pulse was the most deficient, collapsing under pressure; the kidney pulse was also weak and secondarily deficient; the spleen pulse was excessive; and the remaining pulses were within normal limits.
Based on meridian differentiation of the symptoms, the hu voice in the five voices, eye fatigue, and stress were interpreted as variations of the Liver Wood meridian. The bladder as the site of onset and heaviness in the lower body were considered variations of the Kidney Water meridian. The shang tone in the five tones, cough-variant asthma, pale coloration of the skin, and a preference for pungent foods were interpreted as variations of the Lung Metal meridian. Overeating, gastric discomfort and distension, excessive rumination, and a preference for sweet foods were considered variations of the Spleen Earth meridian. Based on these comprehensive findings, the pattern was diagnosed as a Liver deficiency pattern. There was no marked predominance of any specific pathological pattern, and considering that the patient was female, the treatment side was determined to be the right side. As several effective antibiotics remained available even in the event of cystitis onset, the prognosis was considered favorable. Treatment was carried out with the assumption that continuous acupuncture therapy could contribute to the prevention of cystitis.
At the first treatment session, contact needling was performed as the root treatment using a silver needle (length 40 mm, diameter 0.16 mm). Tonification was applied to Rght-sided-LR5, where the pulse was most regulated. Thereafter, right-sided acupoints are denoted as “R-” and left-sided acupoints as “L-”. On pulse diagnosis, the contour of the liver pulse became clearer. Tonification was similarly applied to R-KI3. On abdominal diagnosis, increased skin tension was observed. As pathogenic factors were detected in the pulses of the gallbladder, stomach, large intestine, and triple burner meridians, draining within superficial tonification techniques using contact needling with a stainless steel needle (40 mm, 0.16 mm) were applied to R-GB37, R-ST40, R-TE5, and R-LI6. For the branch treatment, in the prone position, stainless steel needles (40 mm, 0.16 mm) were retained at BL20, BL23, and BL53, which were assessed as deficient. After confirming that the pulse remained stable, the session was concluded. The patient reported relief of back tension following the root treatment.
At the second treatment session (March, year X; Y+2 days), back tension had recurred. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8 and R-KI10. For branch treatment, stainless steel needles (40 mm, 0.16 mm) were retained at L-LR3, R-PC6, and GV19. In the prone position, stainless steel needles (40 mm, 0.16 mm) were retained at BL18 and BL23, and stainless steel needles (40 mm, 0.20 mm) were retained at BL25, BL32, and BL53. At the third treatment session (March, year X; Y+5 days), the patient reported improved sleep and general condition after treatment. Back tension had resolved. She reported discomfort due to overeating. Abdominal diagnosis indicated liver and kidney deficiency; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8, R-KI10, R-KI7, and R-LI1. In addition, draining within superficial tonification techniques were applied to R-GB37, L-BL58, and R-LI6, where pathogenic factors were detected. For branch treatment, in order to further enhance the kidney pulse, needles were retained at L-KI6 and R-LU7, as well as at GV19. One cone of warm-tube moxibustion (Yamashou Ch?an NEO DX, regular type) was applied to LR5. In the prone position, needles were retained at BL18, BL52, BL32, and BL53.
At the sixth treatment session (March, year X; Y+17 days), the patient reported prodromal symptoms suggestive of cystitis. She had perspired and subsequently felt chilled, and reported a persistent sensation of deep coldness even after bathing. Abdominal diagnosis indicated deficiency of the kidney and spleen; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated spleen and kidney deficiency. Based on a combined Kidney and Spleen deficiency pattern, tonification was applied to R-KI3 and L-SP3, while draining within superficial tonification techniques were applied to R-TE5 and R-LI6. For branch treatment, needles were retained at L-KI6 and R-LU7, and one cone of warm-tube moxibustion was applied to SP6. In the prone position, needles were retained at BL20, BL23, BL32, and BL53.
At the eighth treatment session (March, year X; Y+28 days), the patient had developed cystitis five days prior and visited a hospital the following day, where antibiotics were prescribed. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. As it was considered that kidney deficiency alone was insufficient for preventing cystitis, the pattern diagnosis was revised to a Liver deficiency pattern. Tonification was applied to R-LR8 and R-KI3, and draining within superficial tonification techniques were applied to L-GB37, R-ST40, and R-LI6. For branch treatment, in order to further enhance the liver pulse, needles were retained at L-LR3 and R-HT5, and one cone of warm-tube moxibustion was applied to SP6. In the prone position, needles were retained at BL18, BL23, BL53, and BL32, and one cone of warm-tube moxibustion was additionally applied to BL32. As part of lifestyle guidance, a constitutional assessment using the Five Viscera Score was conducted.
At the ninth treatment session (March, year X; Y+31 days), the patient expressed a desire to prevent recurrence of cystitis. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR5, R-KI7, and R-KI3. For branch treatment, needles were retained at R-KI6, R-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at BL18 and BL53, and one cone of warm-tube moxibustion was applied to BL23, BL25, and BL32. Thereafter, ST27, CV3, SP6, BL23, and BL32 for moxibustion were defined as the standard acupoints for the treatment of cystitis.
At the fifteenth treatment session (April, year X; Y+56 days), the patient reported prodromal symptoms of cystitis four days prior, which resolved within approximately two hours after taking Kampo medicine. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR3 and R-KI3, while draining within superficial tonification techniques were applied to R-GB37, R-ST40, and R-TE5. For branch treatment, needles were retained at L-LR3 and L-PC6, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at BL10, GB21, BL18, and BL25, and one cone of warm-tube moxibustion was applied to BL52 and BL32. Notably, warm-tube moxibustion at BL52 had been performed in place of BL23 since the eleventh treatment session (April, year X; Y+42 days). In addition to previously consumed probiotics, the patient was advised regarding the potential immune-enhancing effects of butyrate-producing bacteria.
At the twenty-first treatment session (May, year X; Y+82 days), the patient reported feeling cold and experiencing prodromal symptoms suggestive of cystitis, requesting warming treatment. Abdominal diagnosis indicated deficiency of the kidney and lung; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated kidney and lung deficiency. Based on a Kidney deficiency pattern, tonification was applied to L-KI7 and L-LU9, while draining within superficial tonification techniques were applied to R-ST40 and R-LI6. For branch treatment, needles were retained at R-KI6, R-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. The abdomen was additionally warmed using an infrared heating device. In the prone position, one cone of warm-tube moxibustion was applied to BL18, BL20, BL52, GB25, BL25, BL32, and KI1.
At the twenty-third treatment session (May, year X; Y+86 days), the patient reported abdominal discomfort and prodromal symptoms suggestive of cystitis. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8, R-KI10, and R-KI3, while draining within superficial tonification techniques were applied to R-ST40. For branch treatment, needles were retained at R-LR3, L-PC6, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at GB20, GB21, BL18, and BL25, and one cone of warm-tube moxibustion was applied to BL52 and BL32.
At the thirty-fourth treatment session (August, year X; Y+161 days), the patient reported no concern regarding cystitis. Abdominal diagnosis indicated deficiency of the kidney and spleen; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated kidney and spleen deficiency. Based on a combined Kidney and Spleen deficiency pattern, tonification was applied to R-KI3 and L-SP3, while draining within superficial tonification techniques were applied to R-GB37, R-ST40, and R-LI6. For branch treatment, needles were retained at L-GB41 and R-TE5, and one cone of warm-tube moxibustion was applied to ST27, CV3, SP6, and ST36. In the prone position, needles were retained at BL10, GB20, SI15, and BL20, and one cone of warm-tube moxibustion was applied to GV14, BL23, and BL32.
At the forty-fourth treatment session (October, year X; Y+245 days), the patient reported discomfort suggestive of cystitis. Abdominal diagnosis indicated deficiency of the kidney and lung; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated kidney and lung deficiency. Based on a Kidney deficiency pattern, tonification was applied to L-KI7 and L-LU8, while draining within superficial tonification techniques were applied to R-GB37, R-BL58, R-LI6, and R-TE5. For branch treatment, needles were retained at R-KI6, R-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. The abdomen was additionally warmed using an infrared heating device. In the prone position, needles were retained at Upper-BL10, SI15, and BL25.
At the forty-seventh treatment session (November, year X; Y+273 days), the patient reported prodromal symptoms suggestive of cystitis. Abdominal diagnosis indicated deficiency of the liver, kidney, and spleen; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated kidney and lung deficiency. Based on a Kidney deficiency pattern, tonification was applied to R-KI7 and R-LU5, while draining within superficial tonification techniques were applied to R-ST40 and R-LI6. For branch treatment, needles were retained at R-KI6 and R-LU7, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at BL10, SI15, BL20, and BL25, and one cone of warm-tube moxibustion was applied to BL23 and BL32.
At the fifty-second treatment session (January, year X+1; Y+315 days), the patient reported mild symptoms suggestive of cystitis. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was floating, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8 and R-KI10, while draining within superficial tonification techniques were applied to R-ST40 and R-LI6. For branch treatment, needles were retained at L-KI6, R-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at GB20, GB21, BL18, and BL20, and one cone of warm-tube moxibustion was applied to GV14, BL23, and BL32.
At the fifty-fourth treatment session (January, year X+1; Y+336 days), the patient reported prodromal symptoms suggestive of cystitis. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8 and R-KI7, while draining within superficial tonification techniques were applied to R-BL58, R-ST40, R-LI6, and R-TE5. For branch treatment, needles were retained at R-KI6, R-LU7, L-GB41, R-TE5, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. The abdomen was additionally warmed using an infrared heating device. In the prone position, needles were retained at BL10, SI15, BL18, and BL20, and one cone of warm-tube moxibustion was applied to BL23, BL25, and BL32. The back was also warmed using an infrared heating device.
At the fifty-sixth treatment session (February, year X+1; Y+357 days), the patient reported having developed cystitis in the previous week. She had slept only approximately two hours per night due to a busy schedule two weeks prior. As she was in the premenstrual period, she had been concerned about the onset of cystitis. Abdominal diagnosis indicated deficiency of the kidney and lung; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated kidney and lung deficiency. Based on a Kidney deficiency pattern, tonification was applied to R-KI7 and R-LU9. For branch treatment, needles were retained at R-KI6, R-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at BL10, SI15, BL18, and BL20, and one cone of warm-tube moxibustion was applied to BL23 and BL32.
At the sixtieth treatment session (April, year X+1; Y+406 days), the patient reported prodromal symptoms suggestive of cystitis two days prior. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was sinking, moderate, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8 and R-KI10, while draining within superficial tonification techniques were applied to R-GB37, R-ST40, and R-LI6. For branch treatment, needles were retained at R-KI6, L-LU7, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. The abdomen was additionally warmed using an infrared heating device. In the prone position, needles were retained at SI15, BL18, and BL20, and one cone of warm-tube moxibustion was applied to GV14, BL23, BL25, and BL32. The back was also warmed using an infrared heating device.
At the sixty-fifth treatment session (June, year X+1; Y+462 days), the patient reported no concern regarding cystitis. Abdominal diagnosis indicated deficiency of the liver and kidney; pulse quality was sinking, slow, and deficient; and comparative pulse diagnosis indicated liver and kidney deficiency. Based on a Liver deficiency pattern, tonification was applied to R-LR8 and R-KI7, while draining within superficial tonification techniques were applied to R-GB37 and R-ST40. For branch treatment, needles were retained at R-KI6, L-LU7, R-ST42, and GV19, and one cone of warm-tube moxibustion was applied to ST27, CV3, and SP6. In the prone position, needles were retained at GB21 and SI15, and one cone of warm-tube moxibustion was applied to BL23, BL25, and BL32.
The treatment interval was adjusted to twice per month, and as no recurrence of cystitis was observed for four months despite the extended interval, preventive treatment for cystitis was concluded.
In discussion, the present case is considered to represent recurrent cystitis characterized by repeated episodes of acute uncomplicated cystitis, as the patient had no underlying diseases and experienced more than three episodes per year. Although acute cystitis is generally treatable with antibiotics, repeated episodes in this case led to antimicrobial resistance, resulting in reduced efficacy and a limitation in available antibiotic options. Therefore, acupuncture treatment was administered with the aim of preventing cystitis and improving susceptibility to recurrence, thereby reducing the need for antibiotic administration.
To clarify the effects of acupuncture treatment, the temporal changes in number of treatment and symptoms are shown in Figure 1. The horizontal axis represents the period after the initiation of treatment, while the vertical axis indicates the number of treatments per month, the number of prodromal symptoms suggestive of cystitis, and the number of cystitis episodes. The number of treatments per month decreased from once every 9 days to once per month. The number of prodromal symptoms fluctuated between 0 and 2-3 episodes per month; however, during the summer period, there were sustained intervals with no symptoms. Despite the reduction in treatment number, the number of prodromal symptoms remained largely unchanged, suggesting that improved immune function may have allowed for a reduction in treatment number.
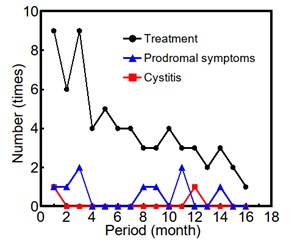
Fig. 1 Number of treatment and symptoms
The second episode of cystitis occurred 12 months after the first episode, indicating that although immune function may have improved, the patient remained susceptible to cystitis during the winter season when the body is more prone to cold exposure. Prior to treatment, cystitis occurred once every 3-4 months, and prodromal symptoms appeared monthly. In contrast, after the initiation of acupuncture treatment, the number of cystitis decreased to once every 12 months which is less than one-third), and prodromal symptoms decreased to 9 episodes over 17 months which is approximately one-half, suggesting that acupuncture treatment contributed to the prevention of cystitis.
This section discusses the root treatment. At the eighth treatment session, it was considered that treatment based on a Kidney deficiency pattern might increase the likelihood of cystitis onset; therefore, treatment was instead conducted based on a Liver deficiency pattern. Accordingly, the distribution of pattern diagnoses used in the root treatment was examined. The proportions were as follows: Liver deficiency pattern, 66%; combined Liver and Spleen deficiency pattern, 5%; Kidney deficiency pattern, 18%; and combined Kidney and Spleen deficiency pattern, 11%. When summarized, the overall proportions were 71% for Liver deficiency patterns and 29% for Kidney deficiency patterns, indicating that treatment based on a Liver deficiency pattern was more frequently applied. These findings are consistent with those reported in Case Studies of Denmei Shudo [10], which noted that Liver deficiency patterns are most common, with additional occurrences of Kidney and Lung deficiency patterns. Furthermore, the distribution of pattern diagnoses at the time of treatment when prodromal symptoms of cystitis appeared was analyzed. The results showed that Liver deficiency accounted for 55% (6 instances), while Kidney deficiency accounted for 45% (5 instances). The relatively higher proportion of Kidney deficiency patterns during prodromal episodes suggests that factors such as sleep deprivation may have contributed to Kidney deficiency, and that treatment targeting Kidney deficiency alone may not have sufficiently addressed underlying conditions such as fatigue and inadequate sleep, ultimately leading to cystitis onset. These findings suggest that although the patient’s condition generally followed a Liver deficiency pattern, a shift to a Kidney deficiency pattern may indicate an increased risk of cystitis onset. Therefore, it is important to inform the patient of this risk and to provide guidance on daily self-care practices to prevent cystitis, particularly when signs of Kidney deficiency are present.
This section discusses treatment using the Eight Confluent Points of the extraordinary meridians. As part of the branch treatment, KI6 and LU7, two of the Eight Confluent Points, were used from the third treatment session onward. In cases of a Liver deficiency or Kidney deficiency pattern, these points were primarily selected when the Kidney pulse remained insufficient after the root treatment. KI6 is associated with the Yin Qiao Mai which is indicated for conditions such as coldness in the lower extremities, knee joint pain, upward rushing sensations, reproductive and sexual dysfunction, and neurosis [13]. It is considered to present symptoms similar to those of the Kidney meridian and is used in cases where tonification or reduction of the Kidney meridian alone is insufficient, suggesting its applicability when the Kidney pulse is inadequate. LU7, associated with the Ren Mai, is indicated for disorders of the reproductive organs, bladder diseases, upward rushing sensations, and neurosis. It is also indicated for disorders due to excess yin and various symptoms along the midline from the lower abdomen upward. As cystitis is a bladder disease and the bladder is anatomically located along the midline of the lower abdomen, LU7 is considered potentially effective for cystitis. According to Shinkyu Shuei, Volume 5, the principal indications of KI6 include cold pain during urination, dysuria with difficulty and obstruction, and bladder qi pain, in which symptoms of cystitis are included. The described treatment method involves first selecting KI6, followed by LU7. Initially, the principal point corresponding to the main symptom is needled, followed by points located at affected regions according to the condition. The treatment proceeds along the meridian flow to regulate qi and eliminate pathogenic factors. If symptoms persist, additional points such as He Water points are selected, and further points may be added as necessary. Needles are retained until qi is regulated, allowing communication between upper and lower regions, and are removed after the patient experiences relief. In the present case, KI6 was needled first, followed by LU7, in accordance with this method. The principal indications of LU7 include urinary retention, in which symptoms of cystitis are included. The described treatment method involves selecting LU7 first, followed by KI6. The extraordinary meridians are considered a highly effective therapeutic concept applicable to a wide range of clinical conditions, regardless of whether they are acute or chronic, and are capable of producing simple and accurate therapeutic effects [14]. Therefore, the use of the Eight Confluent Points in this case is considered to have contributed to the prevention of cystitis.
This section discusses treatment using warm-tube moxibustion. From the ninth treatment session onward, warm-tube moxibustion was applied to ST27, CV3 [5, 7, 9], SP6 [5, 6, 10], BL23 [5, 6, 10], and BL32 [5, 9, 10] as standard acupoints, with the aim of warming the pelvic region. CV3, SP6, BL23, and BL32 are frequently described in the literature as treatment points for cystitis. In addition, these acupoints overlap with those commonly used for dysmenorrhea and fertility support. Based on the patient’s report that she tended to experience prodromal symptoms of cystitis prior to menstruation, cystitis in this case was considered to be associated with the menstrual cycle. Therefore, acupoints related to menstrual conditions were selected with the expectation that they would also be effective for preventing cystitis. These findings suggest that the standard acupoints used in this study, ST27, CV3, SP6, BL23, and BL32 may be effective for the prevention of cystitis.
This section discusses the lifestyle guidance provided. At the eighth treatment session, a constitutional assessment using the Five Viscera Score was conducted as part of lifestyle guidance, and the proportions of qi deficiency, qi stagnation, blood deficiency, blood stasis, yin deficiency, yang deficiency, fluid retention, yang heat, and phlegm-fluid retention were evaluated. In this assessment, scores of 50% or higher were defined as “existing disease,” while scores between 30% and 50% were defined as “pre-disease.” No category met the criteria for existing disease. The categories classified as pre-disease were blood deficiency (41%), yang heat (40%), qi deficiency (39%), qi stagnation (38%), blood stasis (35%), and fluid retention (32%). The patient was provided with explanations regarding the characteristics of each pattern, appropriate lifestyle modifications, and recommended and restricted foods [15]. As there were no marked differences among the scores, the patient was advised to focus on daily self-care practices based on the patterns most closely matching her condition among the major categories identified. In addition, as part of lifestyle guidance, the patient was informed at the fifteenth treatment session about the potential immune-enhancing effects of butyrate-producing bacteria. Butyrate, produced by these bacteria, plays an important role in immune regulation, particularly in intestinal immunity, with one of the main mechanisms being the induction of regulatory T cells (Treg), which suppress inflammation [16]. The patient reported taking supplements containing butyrate-producing bacteria, and such supplementation is expected to contribute to the prevention of cystitis through enhancement of immune function. Taken together, these findings suggest that lifestyle guidance also contributed to the prevention of cystitis.
As demonstrated in this case, acupuncture treatment combining root treatment based on Liver and Kidney deficiency patterns with the use of the Eight Confluent Points, warm-tube moxibustion, and lifestyle guidance may be effective for the prevention of cystitis.
In summary, acute cystitis can generally be treated effectively with antibiotics; however, in recurrent cases, antimicrobial resistance may develop, making prevention of recurrence essential. Therefore, acupuncture treatment was administered with the aim of preventing cystitis and improving susceptibility to recurrence. This report presented a case of acupuncture treatment for the prevention of cystitis. The patient had first developed cystitis 34 years earlier and, over the past 3 years, had experienced episodes at a frequency of once every 3-4 months. As the available antibiotic options had become limited, she sought treatment to prevent further episodes without relying on antibiotics. At the first session, a Liver deficiency pattern was diagnosed. Subsequently, treatment was expanded to include needling of the Eight Confluent Points, KI6 and LU7, as well as warm-tube moxibustion at ST27, CV3, SP6, BL23, and BL32, which were defined as standard acupoints for cystitis. By the sixty-fifth treatment session, the treatment interval had been extended to twice per month, and as no recurrence of cystitis was observed for four months, preventive treatment was concluded. Following the initiation of treatment, the number of cystitis decreased to less than one-third, and the number of prodromal symptoms decreased to approximately one-half, suggesting the potential of acupuncture treatment in preventing cystitis. Furthermore, a shift from a Liver deficiency pattern to a Kidney deficiency pattern was associated with an increased risk of cystitis onset, highlighting the importance of lifestyle guidance. Acupuncture treatment combining root treatment based on Liver or Kidney deficiency patterns with the use of the Eight Confluent Points, warm-tube moxibustion, and lifestyle guidance may be effective for the prevention of cystitis.
References
[1] Takeshi Nishino. Study on mechanisms of antimicrobial resistance. Jpn. J. Chemother. 2014; 62(2): 177-191.
[2] Nanzando's Medical Dictionary, 18th ed., Nanzando, 1998: 461, 1941, 2025.
[3] Japan College Association of Oriental Medicine edited Clinical Medicine Detailed Exposition, 2nd ed., Ishiyaku Pub., 2015: 89-90.
[4] Clinical Nursing Encyclopedia, 2nd ed., Medical Friend, 2000: 1882-1886.
[5] Acupuncture and Moxibustion, 11th ed., Kankando; 1985: 697-699.
[6] Commentary on Valuable Records on Acupuncture and Moxibustion. Idononippon, 2007: 97, 105, 122, 170.
[7] Essence of Acupuncture and Moxibustion. Idononippon. 1935: 296.
[8] Medical Dictionary of Acupuncture and Moxibustion. Ishiyama Acupuncture Medical Pub. 1979: 294-295.
[9] Medical Dictionary of Clinical Acupuncture and Moxibustion, 14th ed., Idononippon. 1993: 195.
[10] Case Studies of Denmei Shudo. Idononippon. 2013: 375-379.
[11] Japanese Acupuncture Medicine: Meridian Therapy and Acupoints. Traditional Japanese Medicine. 2015: 79, 103, 151, 152, 157, 299.
[12] Super-rotation Technique and Clinical Acupoints. Idononippon. 2009: 104-106, 136, 168, 179.
[13] Yusen Yamamoto. Study of extraordinary meridians. J. Jpn. Acupuncture & Moxibustion Soc. 1962; 11(3): 30-36.
[14] Yusen Yamamoto. Position of extraordinary meridians in the meridian therapy system. J. Jpn. Soc. Oriental Medicine. 1966; 17(3): 104-106.
[15] Food Guide for Medicinal Cooking and Kampo. Natsumesha; 2013: 19-27.
[16] Yukihiro Furusawa. Commensal microbiota induce colonic regulatory T cells through epigenetic modification. J. Intestinal Microbiology. 2017; 31: 15-22.
(Accepted 6 July 2025)
 Dr. Nobuyuki Otsuka
Dr. Nobuyuki Otsuka
He graduated from Tohoku University in 1985 and completed the first half term of doctoral course of Tohoku University graduate school in 1987.
He was awarded doctor degree in 1997 from Tohoku University.
He established Hotal Ancient medicine Research Institute (HARI) in 1999.
He established Otsuka Clinic for acupuncture and moxibustion after graduated from Meiji School of Oriental Medicine in 2017.
He is engaged in research on oriental medicine such as traditional Chinese medicine, acupuncture and moxibustion, qigong etc.
Affiliation
Hotal Ancient Medicine Research Institute (HARI), Otsuka Clinic
Address
3-8-14 Hotarugaike-nakamachi, Toyonaka, Osaka, 560-0033 Japan
E-mail
hari.otsuka.holding@gmail.com
Submission Guidelines of Hotal Traditional Oriental Medicine Letters
Text PDF-0.1M

Institute Profile
Hotal Ancient Medicine Research Institute
![]() 3-8-14 Hotarugaike-nakamachi, Toyonaka, Osaka, 560-0033 JAPAN
3-8-14 Hotarugaike-nakamachi, Toyonaka, Osaka, 560-0033 JAPAN